First things first. I need to give credit to Dr. Frank for the title – It is a great, honest, straightforward statement on where we believe we are today as radiation oncologists who treat head and neck cancer. I moved to Oklahoma City primarily for the treatment of head of neck cancer.
I believe that we can do better than we do today with IMRT. I believe that we can reduce side effects. If myself or a family member were diagnosed with a head and neck cancer – I would, at a minimum, be evaluated at a proton therapy center. Pretty much every time.
There are cases where I think the benefit is very small. These are exceptions. But in simple terms, those cases are too detailed for me to write out here. In my opinion – and in the opinion of some pretty good people at a cancer facility in Houston, Texas named MD Anderson – proton therapy out performs IMRT or VMAT or anything x-ray based for the management of head and neck cancer.
As of today, there is really strong data showing:
-
Less radiation to the mouth
-
Less toxicity
-
Less feeding tubes
-
Improved ability to return to work
-
Less total cost of care for the management of the disease
Above is a simple photo of the inside of two patients mouths. On the left is an IMRT case showing large ulcers from the radiation. On the right is a far more “normal” appear tongue. The argument against protons is that – the doses are low and so really it doesn’t matter. I think, looking at the pictures and after caring for Head and Neck cancer patients for a few decades that it does.
Head and neck cancer treatment is a very difficult treatment.
I use the phrase – it is a life changing treatment.
The two patients shown have ZERO risk of the cancer being in the front of the tongue – it is NOT a target. IMRT gives “low doses”. Those “low” doses are enough to cause those big sore in the mouth and causes hair to often fall out on the back of the head as shown in the image discussing “Beam Path toxicities” (that is an extreme case of hair loss but it happens). Those are regions where there is zero risk of disease and it should receive zero dose. With Proton Therapy, they do – they receive zero dose.
So – to me – those differences would be enough. But, especially when using protons, physicians, even radiation oncologists, make arguments like… “but does it really help outcomes” or, “it hasn’t been proven in randomized prospective trials” even though they are using a treatment like IMRT or VMAT with no US level 1 randomized prospective data.
Less toxicity leads to less things like feeding tubes. In the pictures shown are two published references to an over 60% reduction and a 50% reduction in feeding tube placement with proton therapy compared to IMRT or VMAT. The standard concurrent drug regimen is cisplatin for many cases and that is a very difficult drug due to toxicity. We must do common sense changes on the radiation side to minimize toxicity so that we can give aggressive proven therapy on the medical oncology side of the treatment – many patients require both and benefit when we give full / aggressive doses.
Proton Therapy = less radiation, less toxicity, and fewer feeding tubes.
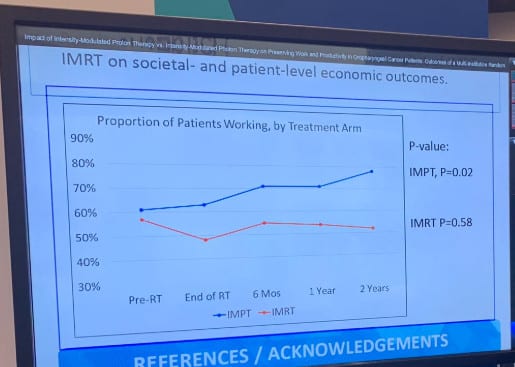
Now lets show data on Quality of Life issues. This was JUST presented about 2 weeks ago at ASTRO 2019. It is randomized prospective data looking at Head and Neck cancer patients showing the percentage of patients who were able to work. Look at just “End of RT” first (the second point moving from left to right). In the proton group – actually 5% more work at the end of treatment than at the beginning. In contrast, IMRT had a 15% drop (nearly 1/4th of the patients) had to stop working through the course of treatment. At 2 years, less IMRT patients work than at diagnosis. At 2 years, 20% more patients work in the proton therapy arm. This is randomized prospective data out of MD Anderson – great work.
Cost data:
I’d love to just reprint what I have on file – but it says confidential and proprietary so I won’t. I’ll summarize the finding of a prospective trial looking at including proton therapy in an insurance coverage plan. The study was a cooperative trial between the University of Texas system, Blue Cross / Blue Shield and MD Anderson looking at management of over 180,000 lives.
The basic assumption was that – protons are more expensive and so costs will be higher but they would be offering better treatment.
The results showed – at the 6 month mark – less total costs for proton therapy. So at a very early time period of only 6 months, even though proton therapy was significantly more expensive than traditional IMRT, the total costs of care was less. Patients went in the hospital less. Patients had fewer feeding tubes. They presented to the ER less etc. etc.
Conclusion
So, for head and neck cancer management: not only is toxicity less, but costs of managing care is less.
If you add in the effect on the workplace, where patients are able to work and contribute to society at a >25% difference, the real difference on “costs” of treatment is far greater. That doesn’t begin to touch the real costs and time commitment of including family members who help care for the patients as they struggle with treatment related toxicity.
For the sake of brevity, I won’t include the recent 2019 University of Washington severe side effect data on 1500 patients (presented ASCO 2019) covering a variety of disease sites including head and neck cancer beyond a link. In this trial patients treated with protons had a 2/3rd reduction in the risk of severe side effects (those that result in ER visits and hospitalizations). Further, there was also randomized prospective data on esophageal cancer presented just two weeks ago showing improvement in side effects in a randomized prospective trial (entry 2).
In my opinion, survival data will follow – it will take time but better short-term outcomes translate to better survival. It has been repeatedly shown across a variety of cancers that when the toxicity profile of the cancer treatment dramatically falls survival improves. It will occur here – it will just take time to show up in the data.
In the meantime, I’ll stick to the published data and say proton therapy results in a less toxicity for head and neck cancer management. And less toxicity with the same cancer outcomes is better.
Medical Director Oklahoma Proton Center