This article applies to locally advanced breast cancers where nodal irradiation is required or cases where IMRT is being considered in breast cancer treatment.
TAKE HOME MESSAGE – Proton plans are better at avoiding the heart than IMRT.
Above are images showing a Proton Therapy plan on the left and an IMRT plan on the right. The heart is circled – it is in the exact same location on both films. The coloring that you see on the right is radiation dose. Radiation dose causes damage to the heart and results in an increase in major cardiac events. There is NO risk of breast cancer spreading to the heart. There is NO reason to deliver any dose to the heart.
You must be your own advocate if you want any reasonable chance of being treated with proton therapy.
Below is great data that is compiled by Legion Healthcare Partners looking at global US payment data. 0.2% were treated with proton therapy – the arrow illustrates the important number. Probably about 10%-15% of patients fall into the group that I am primarily discussing in this article – women with more advanced nodal disease or where comprehensive nodal irradiation is indicated.
Limiting Radiation to the Heart when Treating Breast Cancer
For me personally, breast cancer and limiting dose to the heart and blood vessels has been a passion for a few decades.
Special shout-out to Dr. Tom Buchholz. This study that I worked on was certainly not my idea as a resident at MD Anderson; it was his. He was one of the three leads on the breast service back in the day with Marsha McNeese and Eric Strom and together we published the small study below. It is one the first papers published looking at radiation doses delivered to the various blood vessels of the heart. There are a few maybe earlier looks, but not many.
From this paper I wrote in 2001, note the dose to heart structures – 20Gy, 30Gy, 40Gy – “scatter” being less than 7 Gy. (Protons give ~4Gy max – not 40 Gy)
Relationship Between Radiation to the Heart and Major Coronary Events
Quickly we will fast-forward to 2013 when the Darby paper was published in the New England Journal of Medicine looking at radiation dose to the heart and the linear relationship to of dose to major coronary events.
This is really a landmark paper. It shows a few important things.
- There is no safe lower threshold – going all the way down to doses below 2 gy showed an increase in the rate of major coronary events.
- As shown in the image on the right, it was consistent at all ages and radiation increased your risk whether or not you had existing risk factors.
- Every gray (unit of radiation dose) results in an increase of 7.4% of your of suffering a major coronary event.
Moving forward, we reach 2018 where the American Heart Association released its first ever commentary on the management of a different disease entity. Below I’ve copied the conclusion – it’s pretty readable.
Today we have more information than ever available on the topic of breast cancer and the importance of reducing the long term risk of cardiac toxicity.
And it is finally beginning to gain more and more recognition in the medical community as an increasingly important measure. In simple terms, as cure rates increase; reducing long-term toxicity – including cardiac toxicity becomes more and more important. The image below is from ESC Congress in Paris – held August 31st – September 4th, 2019.
Below is a brand new study looking at Proton Beam Radiation for patient requiring regional nodal treatment for breast cancer – It comes out of MGH and was published in the Journal of Clinical Oncology. It has just been released in the last 2 weeks on August 26th, 2019.
It shows several important items:
- Proton therapy is safe and effective for the treatment of breast cancer.
- Local control was outstanding and overall survival was very high
- Doses to the heart, coronary vessels, and lung – essentially disappear – a literal fraction of what IMRT can accomplish.
Study from the American College of Cardiology
For the next article, we go back into the field of Cardiology – The Journal of the American College of Cardiology. Published in June of 2019 (so I guess this one is now getting old 🙂 ).
It looks at LUNG cancer – so it isn’t a breast article per se, but it replicates the Darby data.
If your heart receives a mean dose of 10Gy, at 3 years (very quickly) – there is a 5% difference in your risk of having a major cardiac event with no prior pre-existing coronary disease. Just to refresh – Protons in the paper above delivered 1/20th of that dose to the heart for breast cancer, whereas 10 Gy is a commonly reported number in the radiation literature for the treatment of complex breast cases.
The point above needs to be repeated: The study above shows that at 3 years, more radiation to the heart resulted in a 5% increase in MAJOR Adverse Cardiac Events following radiation therapy for patients with no pre-existing heart disease.
I’ll finish up with two studies published in the past year – both out of Memorial Sloan Kettering – a true top tier institution in our fight against cancer. In the first one, they report there outcomes for breast cancer treated with proton therapy. In the second study, they report outcomes for breast cancer treated with IMRT. I’ve included the articles so the more technical readers can go to the source material and see just how dramatically different the radiation doses are in these two papers.
I’ll just put together a few comparisons now that you have context:
- Mean heart dose: ~11 gy for imrt, 0.7 gy for proton therapy. IMRT gave 15 times the radiation to the heart.
- Ipsilateral lung: basically all the lung on the side of the tumor receives 5gy of radiation with imrt, with proton therapy about 34% recieves 5 gy.
Below are the actual studies that I summarized very briefly above.
The Proton Therapy Data
The IMRT Data
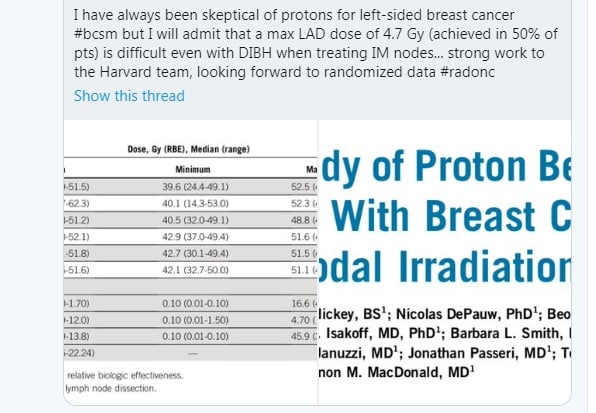
Finally, I’ll leave with a Twitter post – the least scientific thing I probably can use here but it works. First read the tweet.
I put this into this article for a few reasons. In simple terms, I think it summarizes a few pretty common themes in radiation oncology today and attitudes towards proton therapy.
- I believe there has been far too much skepticism towards proton therapy and this re-iterates that thinking. Proton plans are often far superior dosimetry-wise.
- There is acknowledgement that the dosimetry is better but still only 1 in 500 women are sent for proton therapy for breast cancer.
- There’s an argument to delay and wait for randomized data when this person clearly uses DIBH and very likely IMRT based on no randomized data. But it essentially provides a self-serving justification for the lack of a referral to a proton therapy center for cases and very likely, a lack of enrollment in the randomized trial that they are waiting on.
Conclusion
In summary, there are decades of data that I only briefly touched upon that clearly show radiation damages the heart. Radiation to the heart simply results in excess cardiac deaths.
Proton therapy has proven benefits in reducing heart dose for breast cancer when tumors are more advanced and nodal irradiation is required. Even with this information, proton therapy simply isn’t used outside of rare instances.
As a patient, it is very reasonable to expect your physician to be aware of the increasing data and be able to discuss with you which patients they send for proton therapy. You have to be your own advocate as, I believe, there is clear bias where proton therapy is held to a higher standard than many other advances in radiation oncology.
Dr. Mark Storey, MD
Medical Director Oklahoma Proton Center