DISCLAIMER / About the Blog – Please read once if you haven’t.
Protecting the heart during the treatment of breast cancer is a critical component of developing an overall cancer treatment plan for a breast cancer patient.
Before we start the more technical side of the discussion, I’d like to remind everyone of the basics of heart health. These are critical. Don’t let the fear of a cancer diagnosis sidetrack you from the basics. These items are available to everyone and are actionable steps towards long term heart health:
Actionable Items:
- Stop smoking
- Eat a healthy diet
- Stay active and exercise during your treatment
- Be active in managing cholesterol and diabetes.
These are all important and, if you are doing well with these, you can probably do more in these four items (especially if you smoke) than you can by becoming more informed as to treatment associated risks. The other main point to remember is:
For most breast cancer patients, radiation improves survival. It is a critical component of your treatment even though it has side effects.
Now that we have covered the basics, we can look at the treatment aspect of breast cancer management and why this is an important topic for you and your care team to consider.
Proton Therapy can play an important role in reducing heart damage from breast cancer treatment.
Breast cancer and long term heart health are closely linked. The great news of today is that, for all women diagnosed with breast cancer, the 5 year overall survival rate is nearly 90% and the 10 years survival rate is nearly 85%. These are great numbers. We’ve made significant progress in the early detection and treatment of the disease. We have more drugs and targeted treatments available now that we ever had in the past and our results and outcomes continue to improve. As short term results improve, minimizing the long-term effects of treatment becomes critical.
In February of 2018, the American Heart Association actually released a statement on breast cancer stating that it is critical to include long-term heart health in the management of breast cancer.
While we have lots of great treatment options for breast cancer, there are actually several important treatments that have KNOWN significant heart side effects. In fact, if you are 65 years or older when diagnosed with early breast cancer, the predominant cause of mortality is heart disease and not breast cancer.
Types of Breast Cancer Treatments
We’ll just focus on a few breast cancer treatments below that impact heart-health:
- Adriamycin – a chemotherapy, often called the red-devil in infusion suites (chemo rooms). The main toxicity of this drug is heart damage leading to congestive heart failure. It is a great drug for many women and improves survival for women with breast cancer, but definitely affects the heart.
- Herceptin – (or trastuzumab) this is a new targeted treatment against cancers that over express the HER2 gene. Again, it is a great treatment for some women but unfortunately the primary side effect of the drug is cardiac toxicity with a risk of congestive heart failure.
- Radiation – Radiation dose to the heart causes long term damage on some level. There was an important study published on this issue in 2013 showing that for every 1 unit “Gy” of radiation delivered to the whole heart, the risk of a significant heart event increased by 7.4%. So if your heart receives 4Gy, then you have a ~29% greater chance of a significant heart event (ie heart attack that put the patient into the hospital or heart attack that resulted in death).
Note: Surgery is not in the list – it really does good at not causing long term effects on the heart or lungs.
So above I listed three major treatment components that might affect your heart after the treatment of breast cancer. So as a patient which ones can you affect change in. Really that is the question – what can I do to help me do better?
Because, while information and knowledge is good – actionable information is much more valuable. So next, we’ll look at things that you can do to help minimize your risk as you go through breast cancer treatment OR things you can do now that you have the above risk factors to help reduce your current and future risk.
WHAT YOU REALLY CAN’T CHANGE: THE RISK FROM ADRIAMYCIN AND HERCEPTIN
Realistically you can not change the need for these components – many women simply need these components for their treatment. They can be critical components to the successful management of breast cancer. Adriamycin and Herceptin risks are largely not changeable by the patient or doctor. As the doctor, you can perform heart imaging to try and pick healthier patients for these drugs but we really can’t “move the needle in heart health”. Remember the context PLEASE, these drugs even with side effects – help cure / control the breast cancer and lead to LONGER SURVIVAL.
What you can change on some level: Radiation dose to the heart.
The simplest thing to do, if you ask me, is simply to ask a single question of your radiation oncologist:
Patient Actionable Item for Breast Cancer Radiation:
Ask: What is the mean dose to my whole heart?
I think simply by being a knowledgeable patient and being an advocate for your own care by asking this basic question, you have a great ability to impact your heart health. Maybe you are in a great spot and maybe you have a great physician, but simply asking the question and then, as a doctor, having to come back to the patient after your planning is complete to review this number with you – the odds are your heart dose will be lower than if you didn’t ask.
And in simple terms, less radiation dose to the heart is better – always. Lower by any amount leads to less cardiac events.
Just asking is probably a really good step in helping you to get good treatment. So lower is better, but is there a goalpost to aim for?
YES. WITH PROTON THERAPY, MEAN DOSE TO THE HEART IS ABOUT 1GY OR SLIGHTLY LESS (EVEN FOR THE MOST COMPLICATED LEFT SIDED CASES).
Data: So now a bit of data. I’ll reference some recent data out of Memorial Sloan Kettering to give you some scale and scope on differences. Two recent papers were published in 2018 and 2019 – both from the same cancer hospital (consistently ranked 1 or 2 in the national cancer hospital rankings) and it showed a mean heart dose of 13.2 Gy for IMRT (fancy non-proton treatment) compared to 1.0 Gy for Proton Therapy patients for post-mastectomy comprehensive radiation treatments (complicated radiation cases where broad treatment is required). (Ref 1,2)
Let’s think about that: This is a top tier great cancer center publishing heart dose of 13.2 Gy vs 1 Gy for non-proton vs. Proton Therapy treatment. That leads to nearly a doubling of your cardiac risk. Math Warning: 7.4% risk / Gy times 12.2 Gy (the difference) – Greater than 90% increase in cardiac event risk.
FOR COMPLEX CASES, IMRT OR HIGHLY TARGETED X-RAY RADIATION EVEN WITH IGRT, DRAMATICALLY INCREASES YOUR LONG TERM HEART RISK FOLLOWING RADIATION WHEN COMPARED TO PROTON THERAPY.
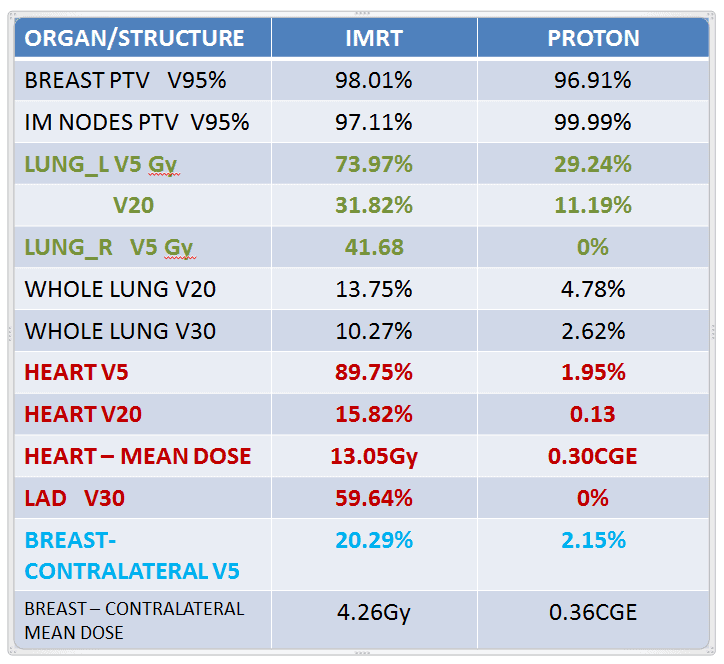
The next images show an example of a comparison plan between photon radiation and Proton Therapy.
WHAT IF PROTON THERAPY ISN’T AVAILABLE IN MY AREA OR MY HEART DOSE SEEMS VERY HIGH?
Remember, you’ve done good. You’re asking questions and pushing your care team to do better. That is done. Other options include finding a facility that does breath hold techniques or has a VisionRT system or some patients benefit from prone breast treatments. These options are far more widespread than Proton Therapy. They can be important ways to improve the plan and lessen dose but realistically, if you don’t get Proton Therapy for an advanced case, your heart dose will likely be between 4 and 10 Gy if treatment is comprehensive even with these techniques.
AGAIN REMEMBER, Even at 13 Gy in the study above, THE BENEFITS OF RADIATION OUTWEIGH THE RISK OF THE TREATMENT. Don’t let anything here let you think you can avoid radiation. It has a PROVEN SURVIVAL BENEFIT even with the heart health risk.
Be an advocate for your own care and ask about heart dose and push for better and remember to control the controllable and push forward as a survivor.
References:
- Luo L, Cuaron J, Braunstein L, Gillespie E, Kahn A, McCormick B, Mah D, Chon B, Tsai H, Powell S, Cahlon O. Early outcomes of breast cancer patients treated with post-mastectomy uniform scanning proton therapy. Radiother Oncol. 2019 Mar;132:250-256. doi: 10.1016/j.radonc.2018.10.002. Epub 2018 Nov 7. PMID: 30414757
- Ho AY, Ballangrud A, Li G, Gupta GP, McCormick B, Gewanter R, Gelblum D, Zinovoy M, Mueller B, Mychalczak B, Dutta P, Borofsky K, Parhar P, Reyngold M, Braunstein LZ, Chawla M, Krause K, Freeman N, Siu CT, Cost Z, Arnold BB, Zhang Z, Powell SN. Long-Term Pulmonary Outcomes of a Feasibility Study of Inverse-Planned, Multibeam Intensity Modulated Radiation Therapy in Node-Positive Breast Cancer Patients Receiving Regional Nodal Irradiation. Int J Radiat Oncol Biol Phys. 2019 Apr 1;103(5):1100-1108. doi: 10.1016/j.ijrobp.2018.11.045. Epub 2018 Nov 30. PMID: 30508620
Dr. Mark Storey MD
Medical Director, Oklahoma Proton Center